Hypothesis / Aims of study
To assess the effects of anticholinergics combined with alpha-blockers in men with lower urinary tract symptoms (LUTS) related to benign prostatic obstruction (BPO)
Study design, materials and methods
We performed a comprehensive search of medical literature, including Cochrane Library, MEDLINE, EMBASE, Web of Science, Chinese Biomedical Literature Database, LILACS, trials registries, other sources of grey literature, with no restrictions on the language of publication or publication status. The date of the latest search of all databases was August 2018. In this systematic review, only randomized controlled trials (RCTs) were included. Inclusion criteria were men with LUTS secondary to BPO, age 40 years or older, and a total International Prostate Symptom Score (IPSS) of ≥ 8. Trials of men with a known neurogenic bladder due to spinal cord injury, multiple sclerosis, or central nervous system disease were excluded. Trials examining medical therapy for men who were treated with surgery for BPO were also excluded. We performed three comparisons: combination therapy versus placebo, combination therapy versus anticholinergic monotherapy, and alpha-blocker monotherapy. The primary outcomes include urological symptom scores, quality of life (QOL), and adverse events, while the secondary outcomes include acute urinary retention (AUR), and surgical intervention. Two review authors independently screened the literature, extracted data, and assessed risk of bias. We performed statistical analyses using a random-effects model and interpreted data according to the Cochrane Handbook for Systematic Reviews of Interventions. We used the GRADE approach to rate the quality of evidence.
Results
We included 23 studies with 6285 randomized men across three comparisons. We only found short term effect (up to 12 months) of combination therapy based on available evidence.
Combination therapy versus Placebo: Based on five studies with 2369 randomized participants, combination therapy may result in an improvement in urological symptom scores (mean difference (MD) -2.49, 95% confidence interval (CI) -4.66 to -0.33; low certainty evidence) and adverse events (risk ratio (RR) 1.69, 95% CI 1.15 to 2.48; low certainty evidence). We are very uncertain about the effect of combination therapy on QOL (MD -0.99, 95% CI -2.18 to 0.20; very low certainty evidence) and AUR (RR 1.94, 95% CI 0.41 to 9.08; very low certainty evidence). None of the studies reported data on number of men with a need of surgical intervention.
Combination therapy versus Alpha-blockers: Based on 22 studies with 4904 randomized participants, we are very uncertain about the effect of combination therapy on urological symptom scores (MD -1.75, 95% CI -3.28 to -0.22; very low certainty evidence), as well as the surgical intervention (RR 6.55, 95% CI 0.79 to 54.00; very low certainty evidence). Combination therapy may improve QOL (MD -0.70, 95% CI -1.06 to -0.34; low certainty evidence), but may not represent a clinically important reduction. Combination therapy may increase adverse events rate (RR 1.35, 95% CI 1.06 to 1.72; low certainty evidence); this corresponds to 64 more adverse events (95% CI: 11 more to 132 more) per 1000 participants. Moreover, combination therapy may result in little to no difference in AUR (RR 1.61, 95% CI 0.77 to 3.35; low certainty evidence).
Combination therapy compared to Anticholinergics: Based on three studies with 1218 randomized participants, we are very uncertain about the effect of combination therapy on urological symptom scores (MD -4.82, 95% CI -12.81 to 3.17; very low certainty evidence), QOL (MD -1.80, 95% CI -2.27 to -1.33; very low certainty evidence), adverse events (RR 1.55, 95% CI 0.82 to 2.90; very low certainty evidence). In addition, combination therapy may result in little to no difference in AUR (RR 0.55, 95% CI 0.11 to 2.68; low certainty evidence).
Interpretation of results
Through literature search, we have also identified three systematic reviews assessing the efficacy and safety of combination therapy with alpha blockers and anticholinergics for men with LUTS/BPH [1-3]. In terms of methodological difference between these reviews and ours, Filson’s review used the IPSS storage subscore as primary outcome, while our review focused on total IPSS. Differing from ours, Xin’s review included some quasi-randomized studies and Kim’s review included both RCTs and non-RCTs. Regarding the review findings, Kim’s review found that combination therapy did not present additional benefit in reduction of IPSS compared to alpha blockers, which is similar to ours. On the contrary, Xin’s review showed combination therapy may lead to a small improvement in IPSS. The important difference between these reviews and ours is that their results assessed the outcomes with a follow-up of at least four weeks, while our review assessed outcomes with a follow-up of at least 12 weeks. Furthermore, our review considered minimal clinically important difference, but they were not. In addition, these reviews did not use GRADE or assess the certainty of evidence on a per-outcome basis.
Concluding message
Combination therapy with anticholinergics and alpha-blockers may be associated with small unimportant or uncertain effects on urologic symptom scores, QOL, and adverse events compared to placebo or anticholinergics monotherapy. However, combination therapy may improve the QOL with uncertain effect on urologic symptom scores, but increase adverse events compared to alpha-blockers monotherapy. The findings of this review were limited by study limitations, inconsistency, and imprecision.
Figure 1
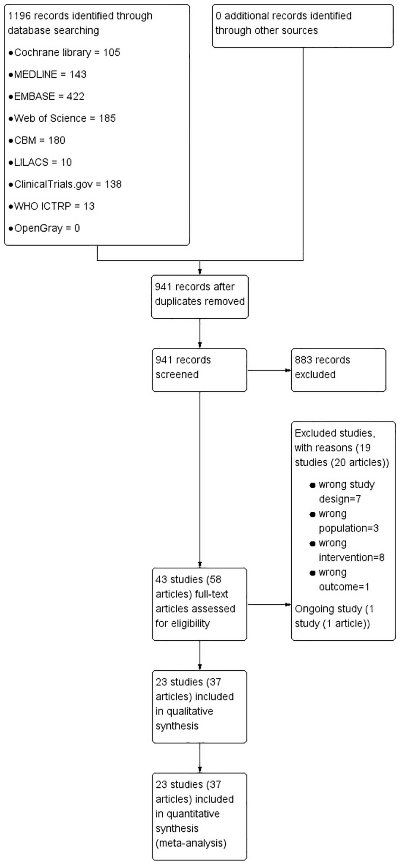
Study flow diagram
Figure 2
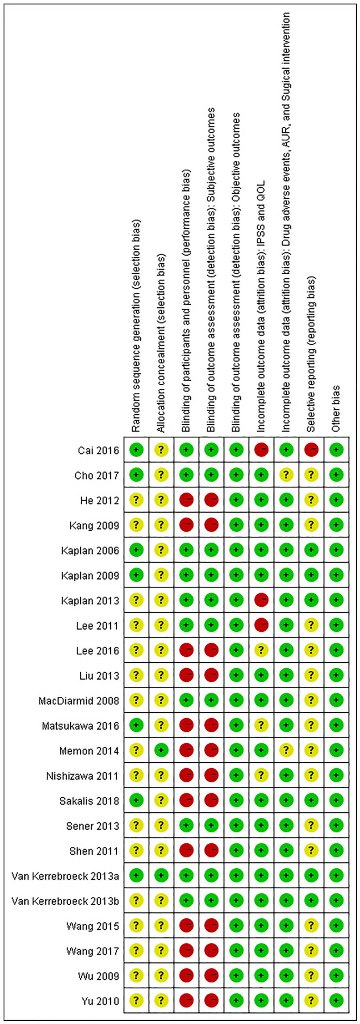
Risk of bias summary
References
1. Filson CP, Hollingsworth JM, Clemens JQ, Wei JT. The efficacy and safety of combined therapy with alpha-blockers and anticholinergics for men with benign prostatic hyperplasia: a meta-analysis. The Journal of Urology 2013;190(6):2153-60.
2. Kim HJ, Sun HY, Choi H, Park JY, Bae JH, Doo SW, et al. Efficacy and safety of initial combination treatment of an alpha blocker with an anticholinergic medication in benign prostatic hyperplasia patients with lower urinary tract symptoms: updated meta-analysis. PloS one 2017;12(1):e0169248.
3. Xin Z, Huang Y, Lu J, Zhang Q, Chen C. Addition of antimuscarinics to alpha-blockers for treatment of lower urinary tract symptoms in men: a meta-analysis. Urology 2013;82(2):270-7.