Hypothesis / aims of study
OnabotulinumtoxinA (Onabot/A) represents the only neurotoxin-A recommended as second‐line treatment for refractory neurogenic detrusor overactivity incontinence (NDOI) in patients with spinal cord injury (SCI) or Multiple Sclerosis (MS), whose efficacy and safety have been demonstrated in powered, multicentre, randomized, controlled trials and in many open label studies [1]. However, large intra-individual variability and/or loss of response along repeat treatments have been variably reported, with rates of failure in up to 40% of cases. [2] Thus, having alternative botulinum toxins for the mentioned indication would be highly warranted. Another botulinum toxin A which is commercially available is IncobotulinumtoxinA, approved by the Food and Drug Administration since 2011 and currently used in other clinical settings.
The aim of the present study was to compare the efficacy, safety and related costs of IncobotulinumtoxinA versus OnabotulinumtoxinA for the treatment of refractory NDOI in patients affected by SCI and MS performing intermittent catheterization (IC).
Study design, materials and methods
We conducted a prospective, national, multicentre, phase III, double-blind, pilot clinical trial, in accordance with the principles set forth in the Helsinki Declaration and approved by the Local Ethics Committee. Sixty-four patients with SCI or MS were randomized to receive 200 U of Incobot/A or Onabot/A (30 intradetrusor injections); 28 patients in Incobot/A and 29 in Onabot/A group completed the study. Primary outcome measure was the non-inferior variation from baseline in daily urinary incontinence (UI) episodes (week 12), with a non-inferiority margin of 1 episode/day. Secondary outcomes measures were changes in Incontinence-Quality of Life (I-QoL) questionnaire, Visual Analog Scale (VAS) to score the bother of symptoms on QoL, urodynamic parameters and occurrence of adverse effects (AEs).
Results
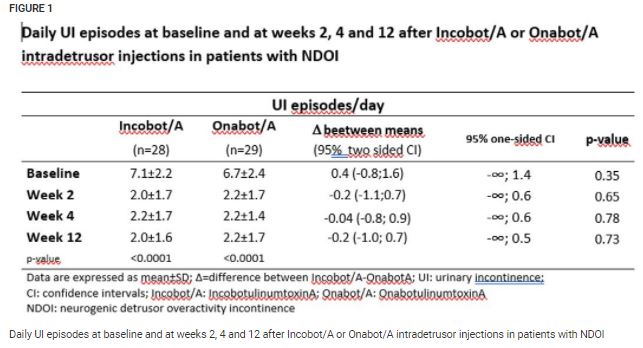
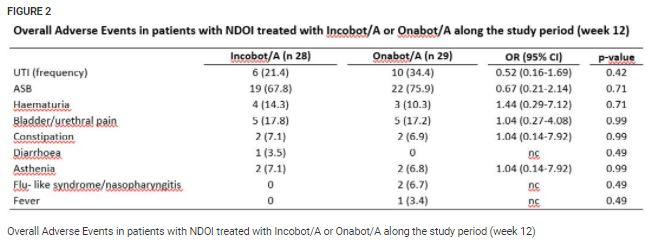
At week 12, mean value of difference in UI episodes/day between the two groups was -0.2 (95% two-sided CI: -1; 0.7) (Fig. 1); the difference in UI episodes/day between the two groups was −0.4 with a higher limit of one-sided 95% CI of 0.2 episodes/day, which was much lower than the non-inferiority margin of 1 episode/day. Total score and subscores of I-QoL, VAS and urodynamics were significantly improved with no differences between the two groups. AEs were similar for both treatments, with urinary tract infection as the most frequent AE (Fig. 2).
Interpretation of results
The novel finding, to our knowledge, of the current study is that, in patients with NDOI resistant to conventional antimuscarinics and performing IC whom we studied, 200 U Incobot/A intradetrusor injections were not inferior to Onabot/A in significantly improving daily frequency of UI, QoL, VAS scores and urodynamic parameters. The beneficial effects were observed just 2 weeks after treatment in both groups of patients and persisted along the whole follow-up period. No risk amount of AEs was observed with the new compound. Incobot/A is a widely used and commercially available botulinum toxin A formulation, intentionally produced to contain only the required therapeutic component, the 150 KDa core neurotoxin. Contrary to Onabot/A, Incobot/A is free from complexing proteins, which are not required for the pharmacological activity. Several randomized, double-blind, head-to-head clinical studies in different clinical settings showed comparable, clinical efficacy of Incobot/A and Onabot/A in terms of time to onset, time to waning, duration of effects and toxicity profile, even if the two botulinum toxins A differ in their specific potency, immunogenicity and biological activity. The low-absent risk of immunogenicity of Incobot/A appears to be particularly useful in patients with neurogenic diseases, who often receive injections to treat multiple different organs’ dysfunction.
Concluding message
In SCI and MS patients with refractory NDOI performing IC, Incobot/A was not inferior to Onabot/A in improving UI, QoL, VAS and urodynamic findings in the short-term follow-up, with comparable AEs
References
Disclosures
Funding None Clinical Trial Yes Registration Number ClinicalTrials.gov NCT03758235 RCT Yes Subjects Human Ethics Committee Ethics Committee of Umbria Helsinki Yes Informed Consent Yes